




“I have lost myself, so to speak”
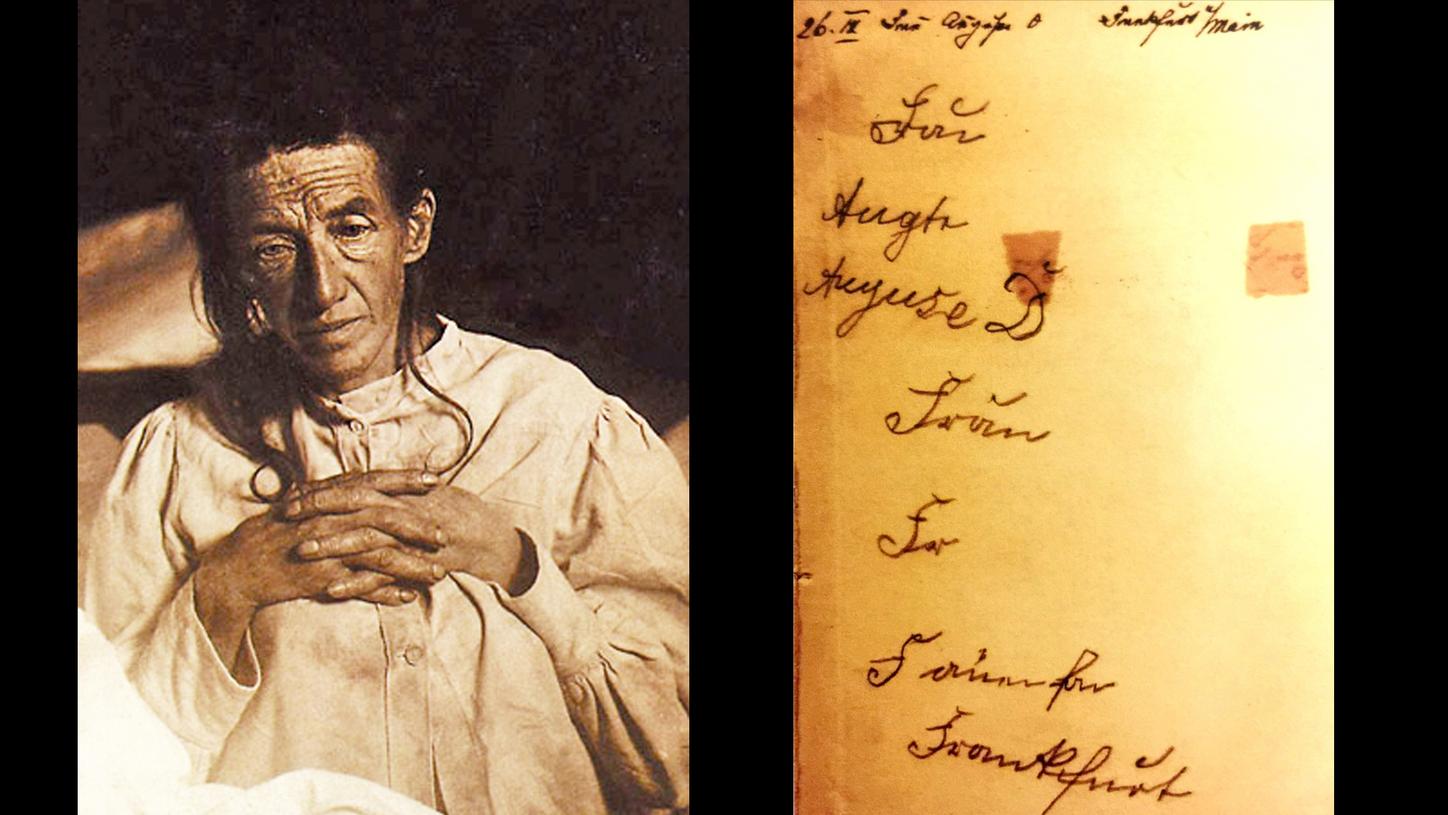
Portrait and handwriting sample from Auguste Deter
But worse than any loss of limb is the failing mind which forgets the names of slaves, and cannot recognise the face of the old friend who dined with him last night, nor those of the children whom he has begotten and brought up.
Decimus Junius Juvenalis, c. 1st and 2nd century AD; translation by George Gilbert Ramsay (1918)
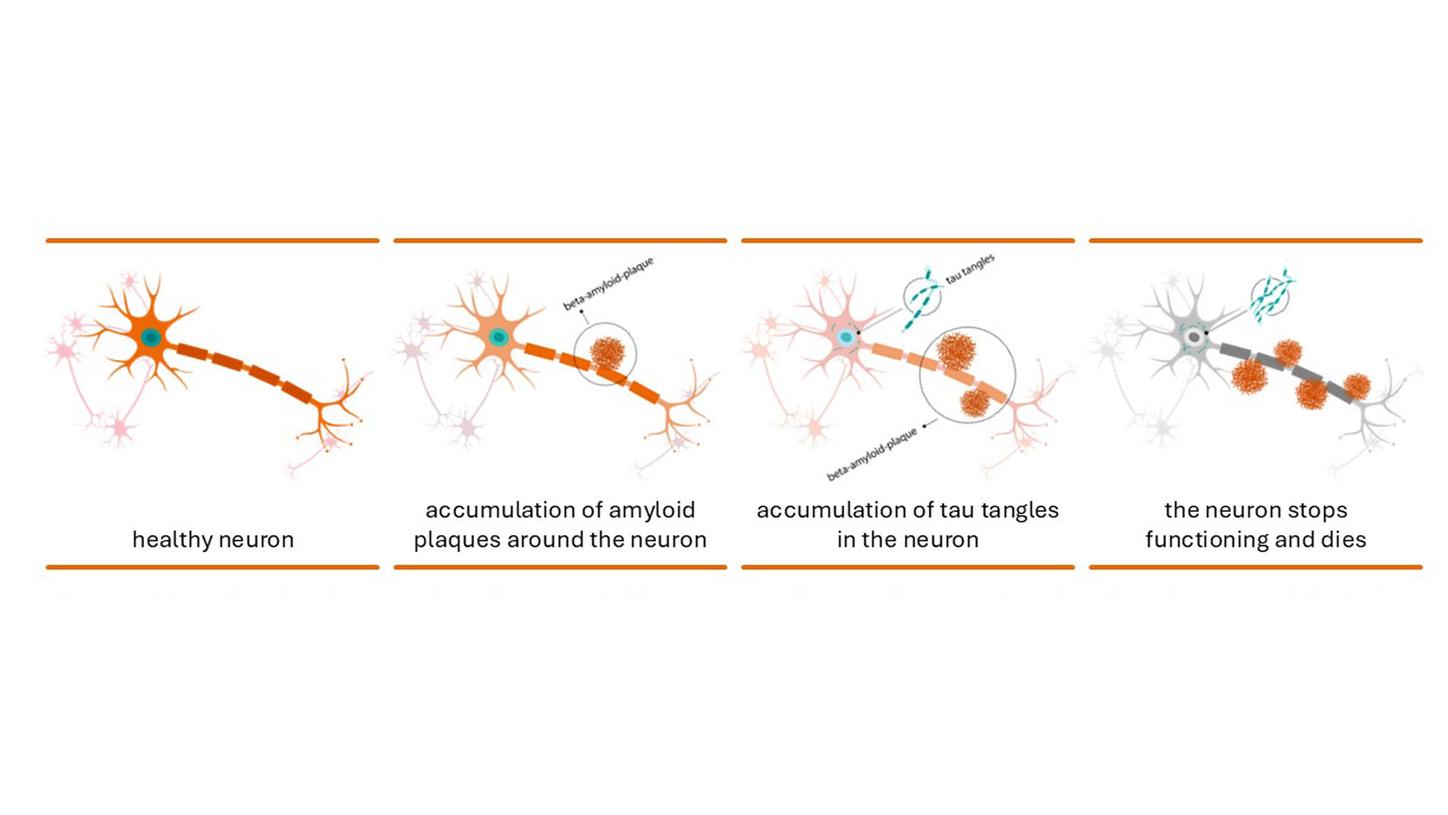
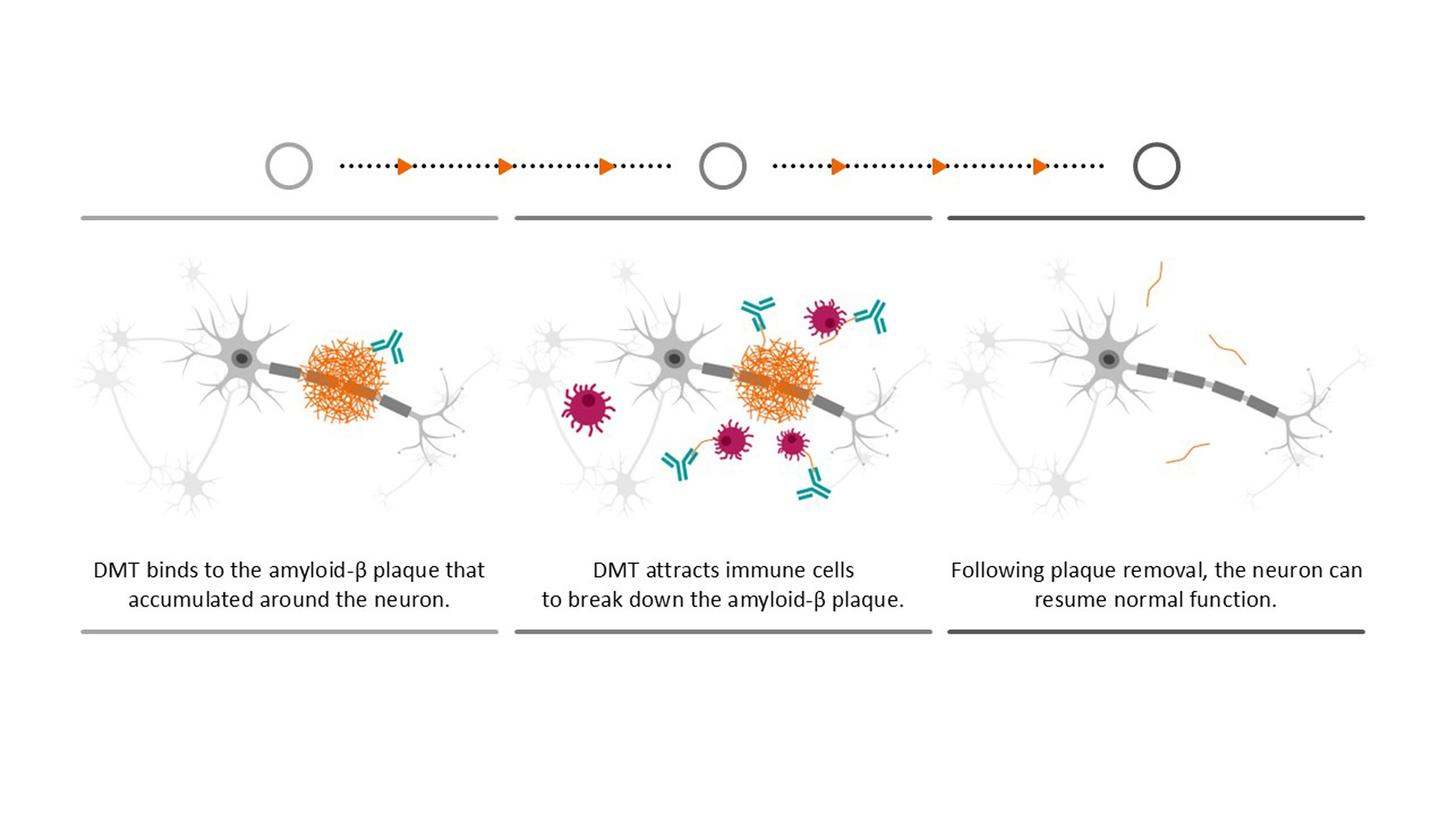
Depiction of nerve cells in a normal brain (left) and of the deposition of amyloid beta plaques and tau fibrils in the brain of an Alzheimer’s patient (middle), which lead to cell death (right),
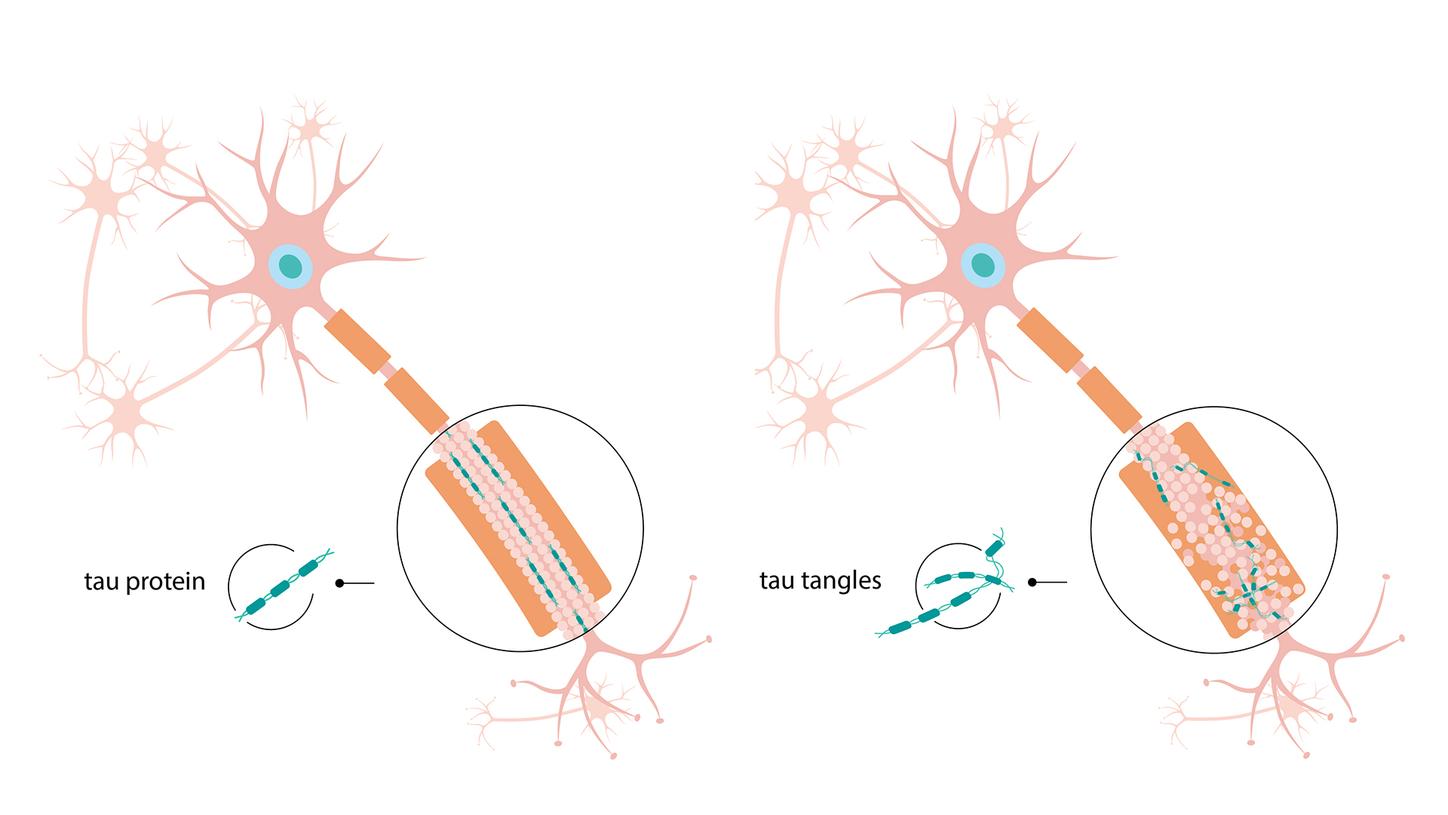
Comparison of a healthy nerve cell (left) and neuronal degeneration (right). In the latter, the tau proteins (turquoise) clump together into tau fibrils that accumulate within the nerve cells.
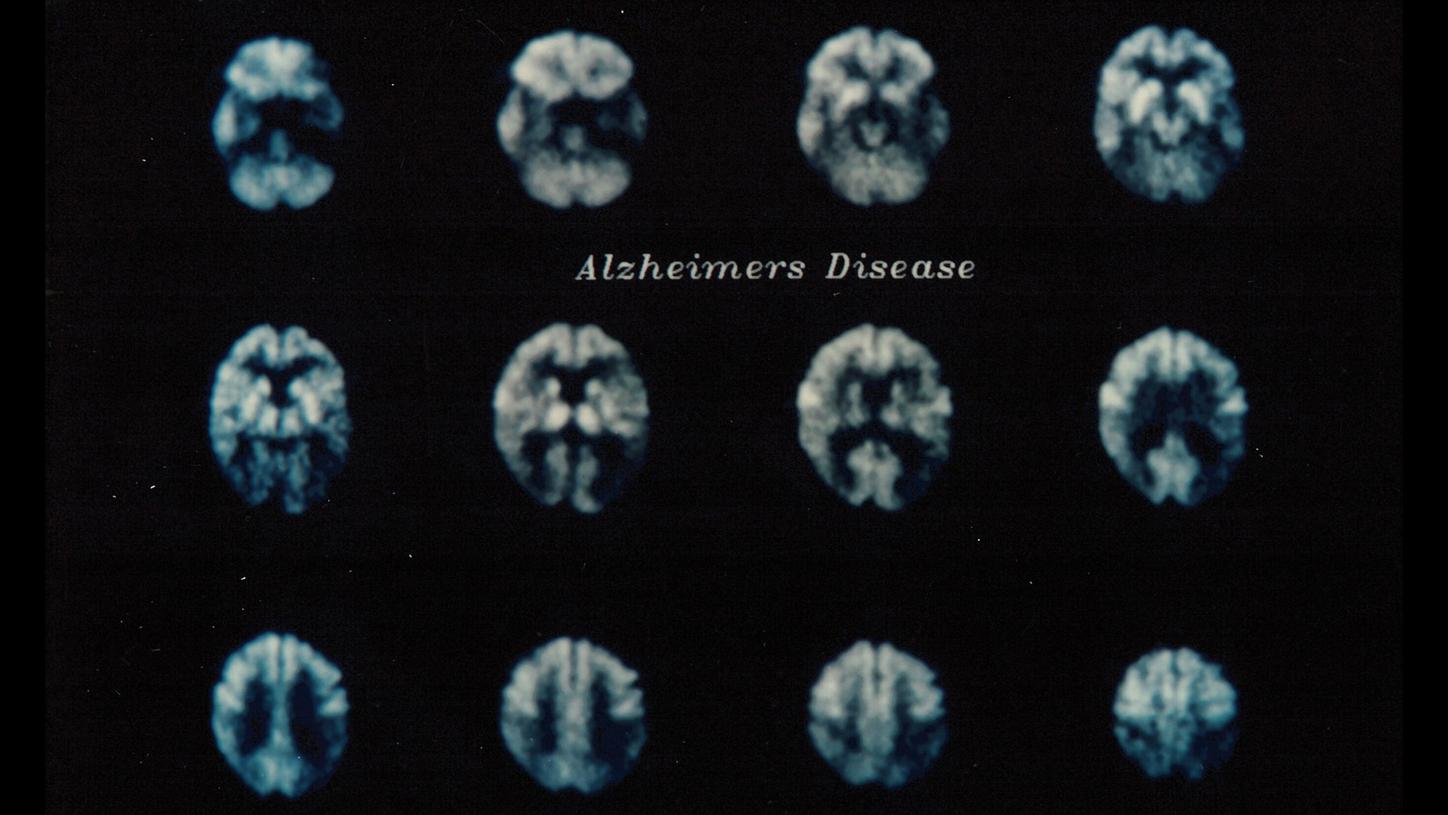
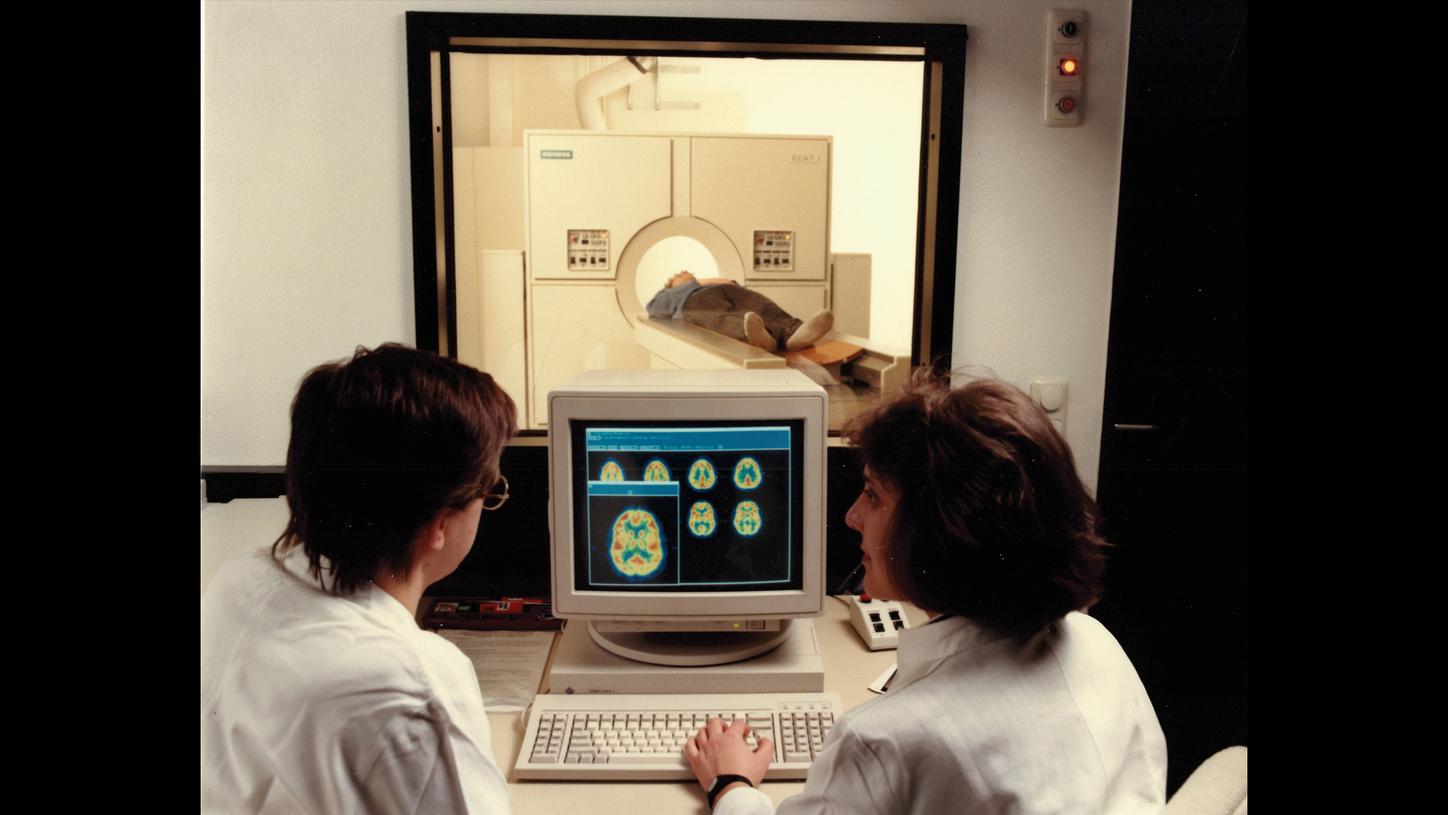
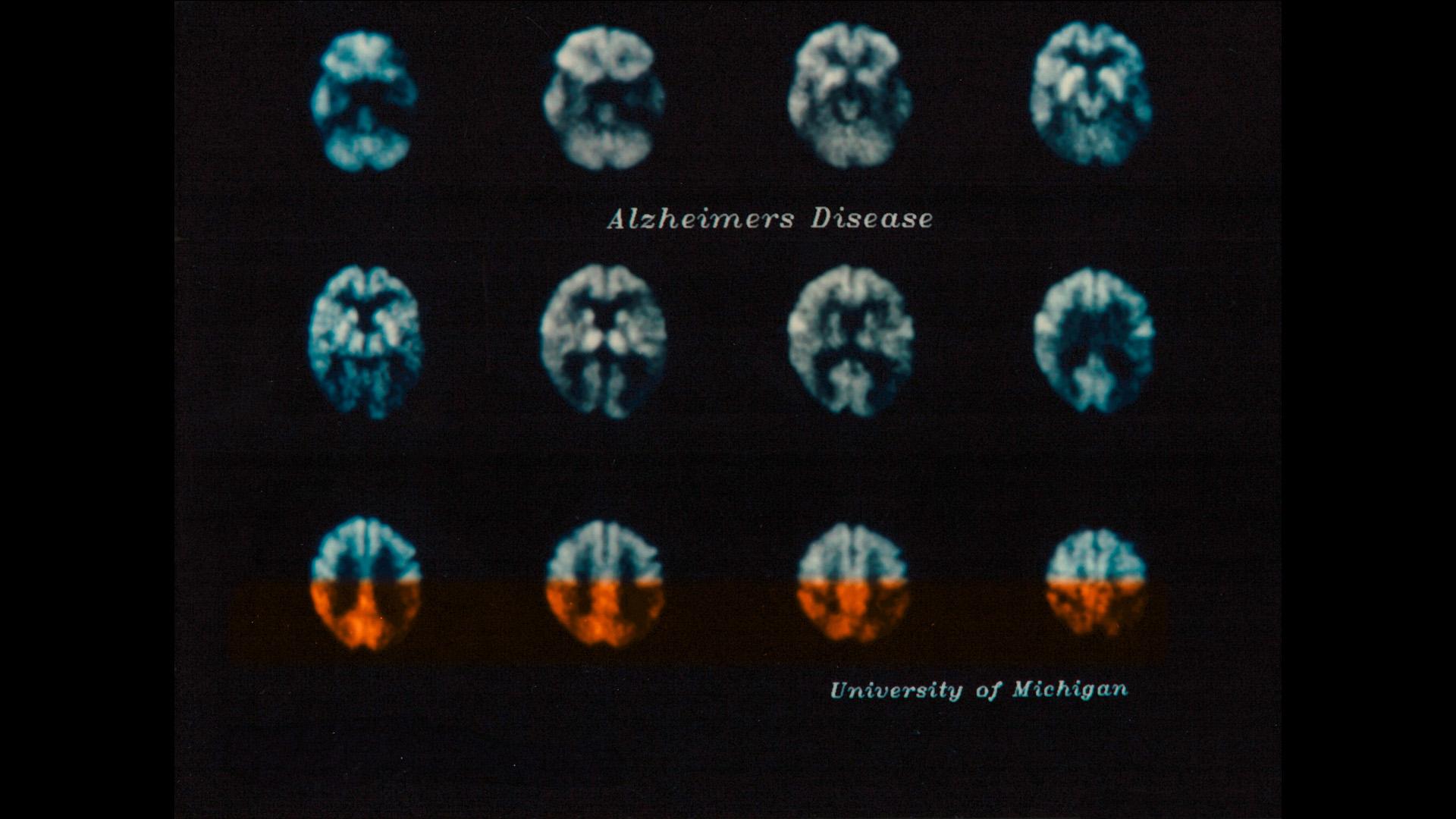
Development of positron emission tomography
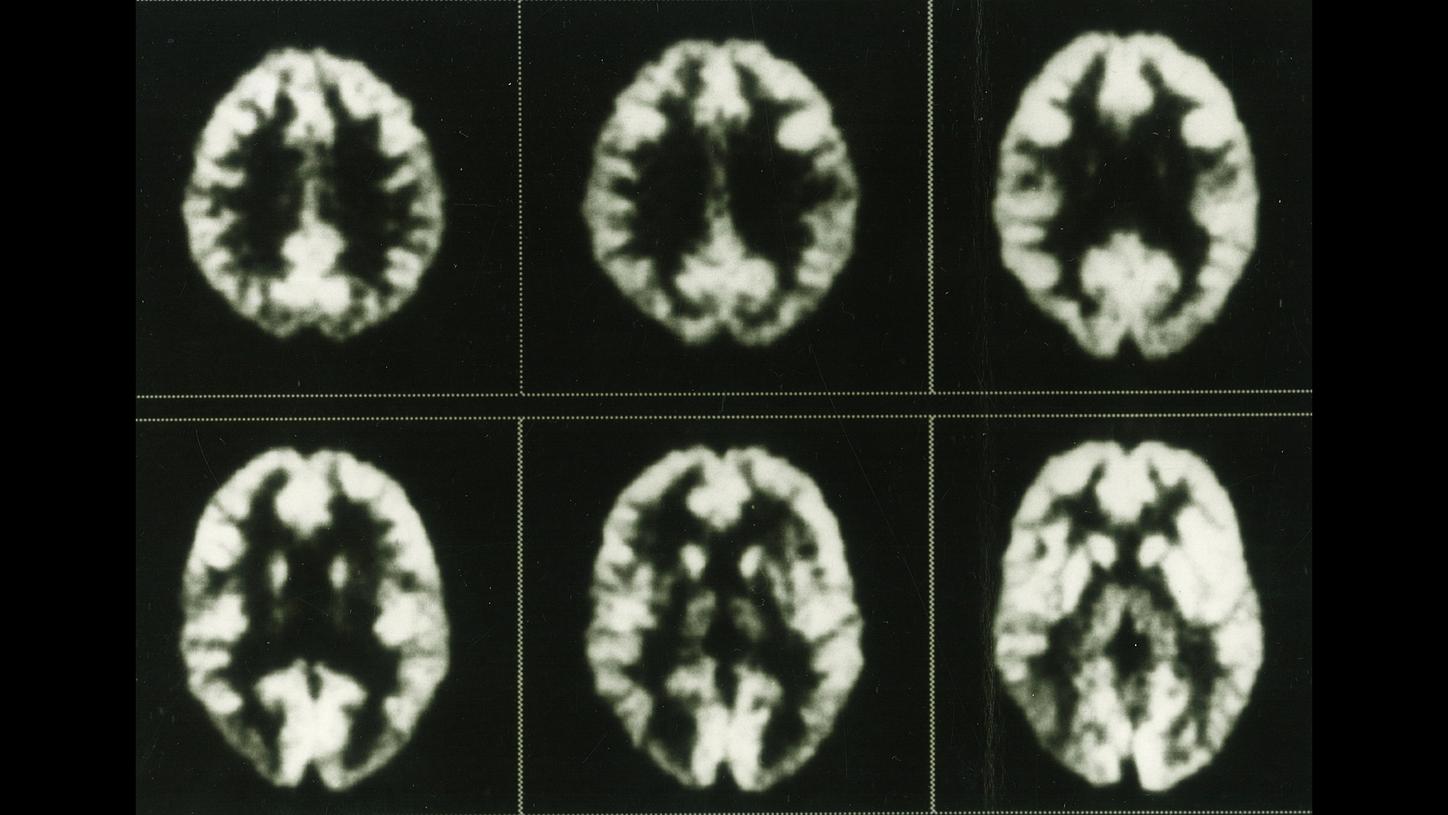
When PET scanners were first developed at the start of the 1970s, even early images from prototypes allowed physicians to observe glucose metabolism in the brain. This series of images, recorded using the ECAT III in the mid-1980s, shows the distribution of fluorodeoxyglucose in a healthy brain.


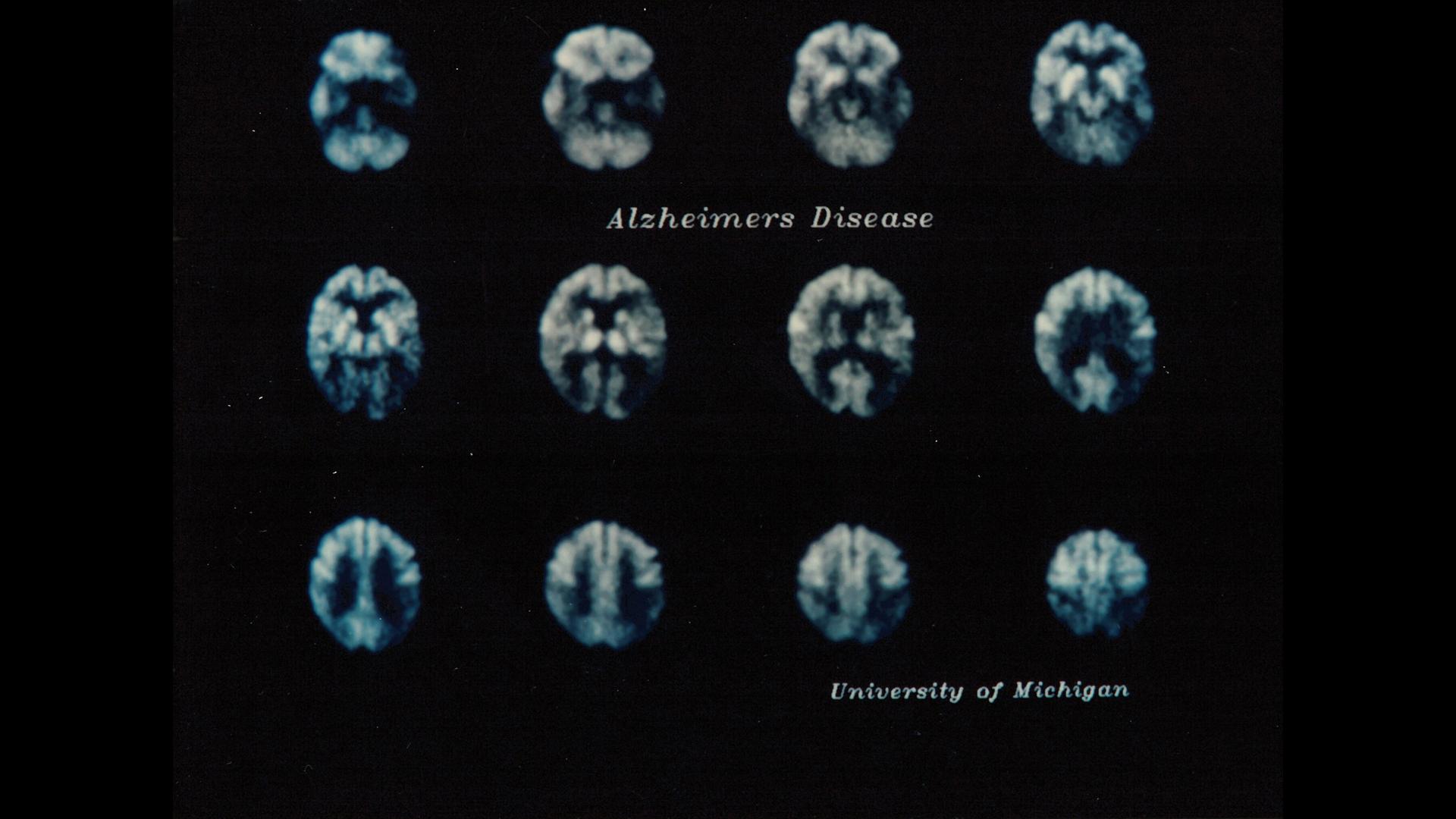
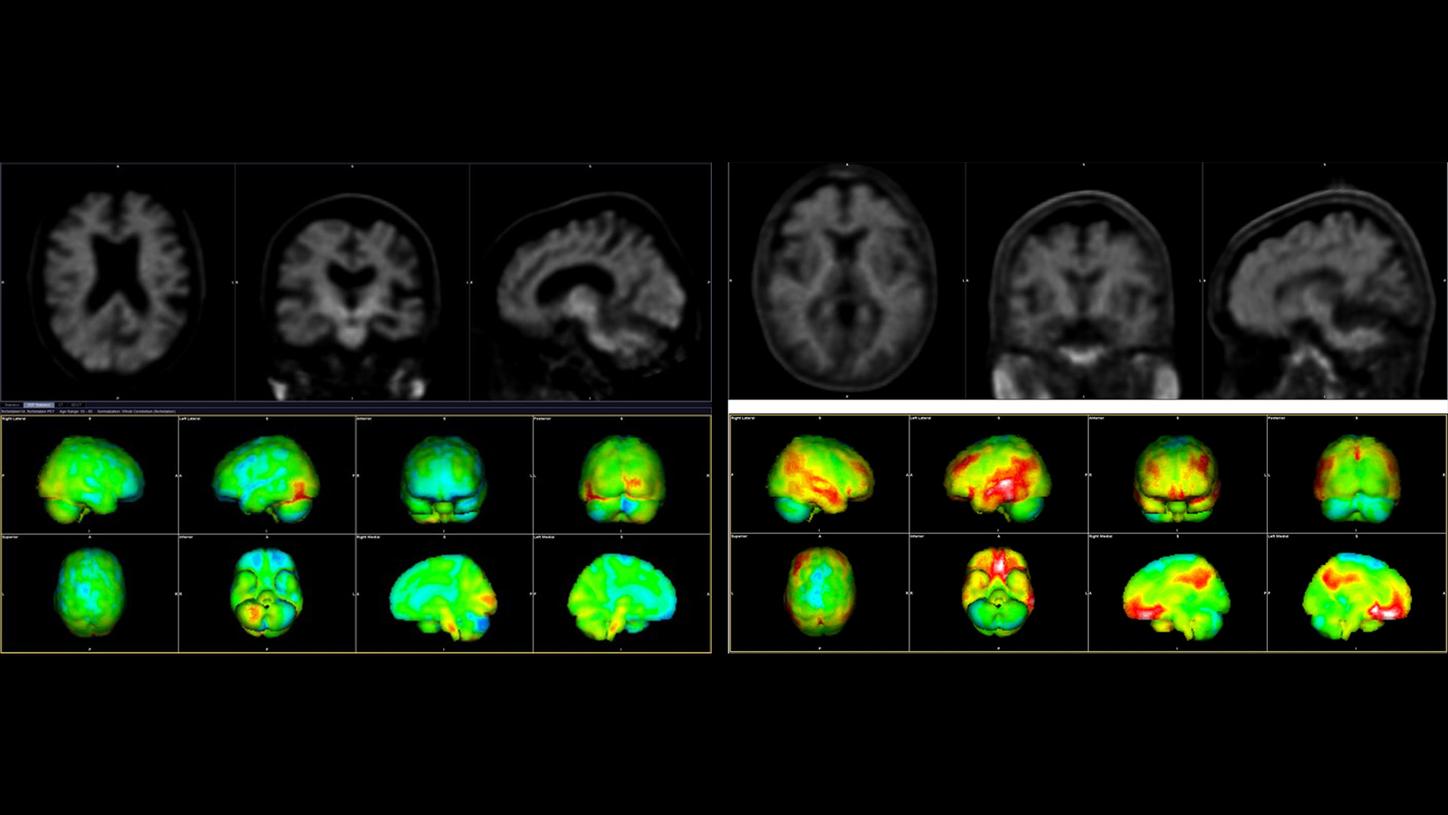
Amyloid PET/CT images to detect amyloid beta plaques (marked in red). The image on the left shows the brain of a healthy older person, while the image on the right shows that of an Alzheimer’s patient.
Data courtesy of Wentworth-Douglas Hospital, Dover, New Hampshire, USA
I now begin the journey that will lead me into the sunset of my life.
Ronald Reagan, 1994

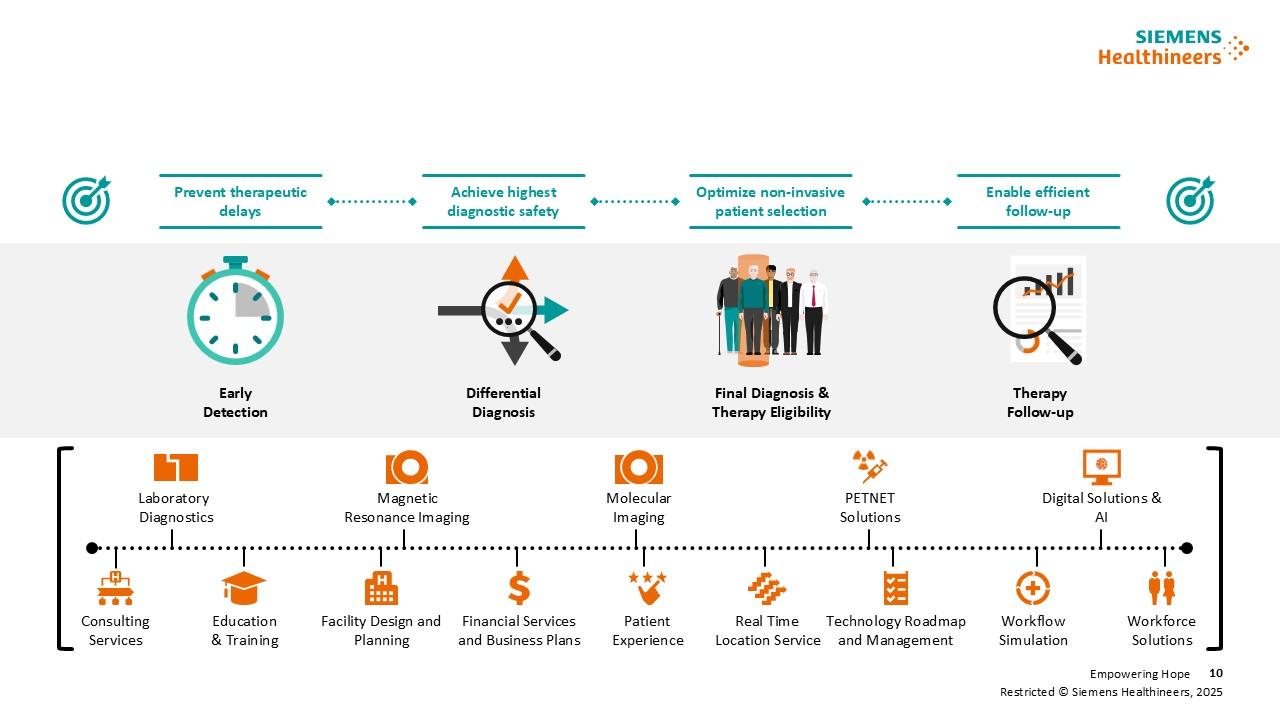
Clinical solutions from Siemens Healthineers support the entire Alzheimer’s care pathway: from early detection to differential diagnostics and treatment monitoring.